Fill a Valid Iowa 470 4299 Template
The Iowa 470-4299 form plays a crucial role in the process of verifying emergency health care services for individuals in need. This form, administered by the Iowa Department of Human Services, is essential for documenting the details surrounding emergency medical situations. It requires information such as the client's name, date of birth, and Social Security number, ensuring that the right individual is being represented. A significant aspect of the form is the consent section, where patients, or their guardians in the case of minors, grant permission for medical providers to share pertinent information with the Department of Human Services. This facilitates a smoother verification process. Additionally, the form includes specific questions aimed at assessing the severity of the medical condition that necessitated emergency care, which can include anything from acute pain to serious bodily dysfunction. Providers are tasked with detailing the dates of service and the nature of the medical emergency, thereby helping to establish the necessity for coverage under Iowa’s Emergency Health Care Services program. Understanding the intricacies of this form is vital for both patients and healthcare providers, as it directly impacts access to essential medical services during critical times.
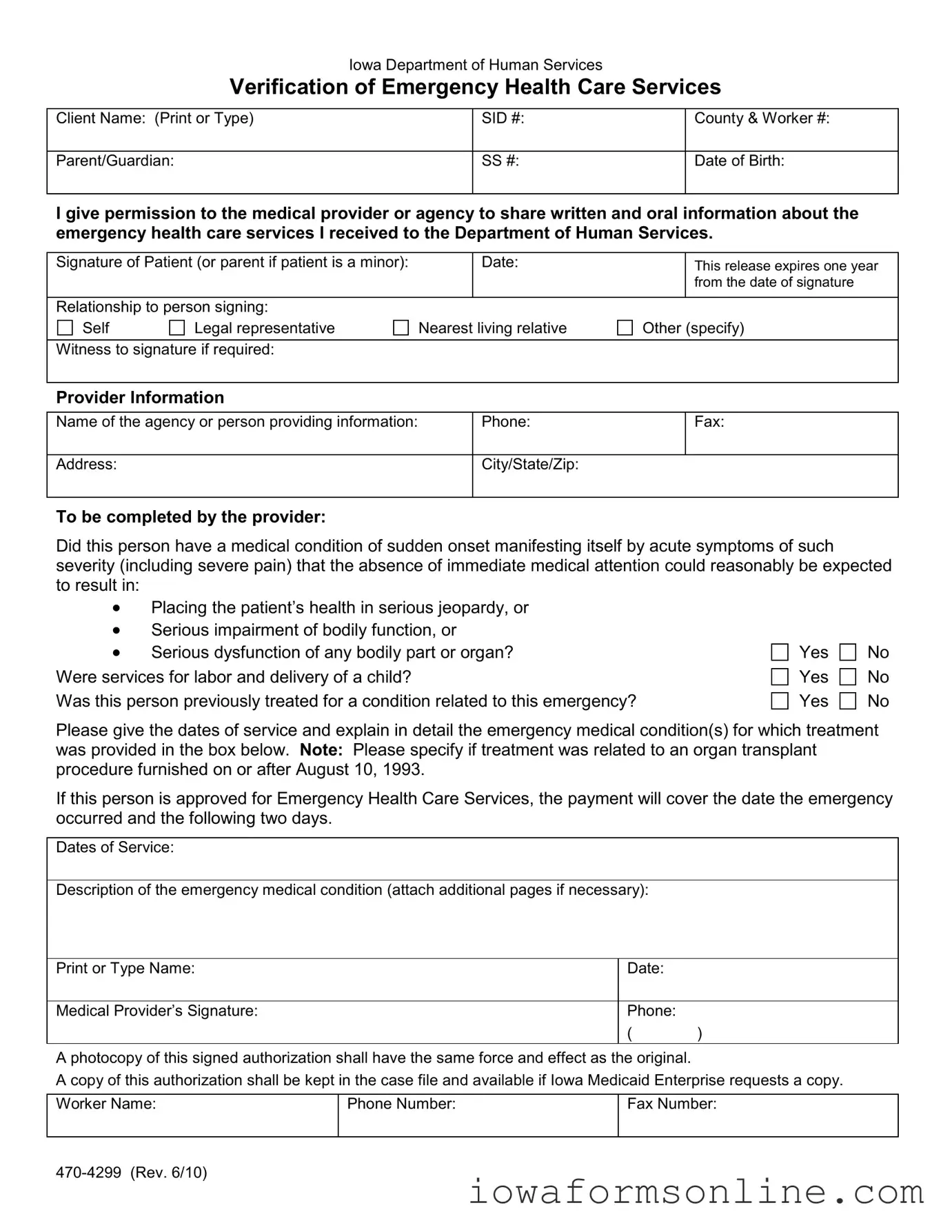
Iowa 470 4299 Preview
Iowa Department of Human Services
Verification of Emergency Health Care Services
Client Name: (Print or Type) |
SID #: |
County & Worker #: |
|
|
|
Parent/Guardian: |
SS #: |
Date of Birth: |
|
|
|
I give permission to the medical provider or agency to share written and oral information about the emergency health care services I received to the Department of Human Services.
Signature of Patient (or parent if patient is a minor): |
|
Date: |
|
This release expires one year |
|
|
|
|
|
|
from the date of signature |
|
|
|
|
|
|
Relationship to person signing: |
|
|
|
|
|
Self |
Legal representative |
Nearest living relative |
Other (specify) |
||
|
|
|
|
|
|
Witness to signature if required: |
|
|
|
|
|
|
|
|
|
|
|
Provider Information
Name of the agency or person providing information: |
Phone: |
Fax: |
|
|
|
Address: |
City/State/Zip: |
|
|
|
|
To be completed by the provider:
Did this person have a medical condition of sudden onset manifesting itself by acute symptoms of such severity (including severe pain) that the absence of immediate medical attention could reasonably be expected to result in:
•Placing the patient’s health in serious jeopardy, or
•Serious impairment of bodily function, or
•Serious dysfunction of any bodily part or organ? Were services for labor and delivery of a child?
Was this person previously treated for a condition related to this emergency?
Yes
Yes
Yes
No
No
No
Please give the dates of service and explain in detail the emergency medical condition(s) for which treatment was provided in the box below. Note: Please specify if treatment was related to an organ transplant procedure furnished on or after August 10, 1993.
If this person is approved for Emergency Health Care Services, the payment will cover the date the emergency occurred and the following two days.
Dates of Service:
Description of the emergency medical condition (attach additional pages if necessary):
Print or Type Name: |
Date: |
|
|
|
|
Medical Provider’s Signature: |
Phone: |
|
|
( |
) |
A photocopy of this signed authorization shall have the same force and effect as the original.
A copy of this authorization shall be kept in the case file and available if Iowa Medicaid Enterprise requests a copy.
Worker Name: |
Phone Number: |
Fax Number: |
|
|
|
Document Attributes
| Fact Name | Fact Description |
|---|---|
| Form Title | Iowa Department of Human Services Verification of Emergency Health Care Services |
| Form Number | Iowa 470-4299 |
| Governing Law | Iowa Code Chapter 249A governs Medicaid services, including emergency health care. |
| Purpose | The form is used to verify emergency health care services provided to clients. |
| Client Information | Includes fields for client name, SID number, county, worker number, and date of birth. |
| Consent Requirement | The patient or their guardian must provide written permission for information sharing. |
| Emergency Definition | The form requires confirmation of a medical condition with sudden onset and acute symptoms. |
| Service Coverage | If approved, payment covers the date of the emergency and the following two days. |
| Expiration of Authorization | The release expires one year from the date of signature. |
Popular PDF Forms
How to Get Resell License - A tax exemption certificate for Iowa businesses, facilitating tax-free procurement of inventory intended for resale.
Iowa 635 0902 - Details about the partnership's organization, including the state or country of origin and the date of organization, are required.
Understanding the significance of a Durable Power of Attorney form is essential, as it provides peace of mind for individuals who want to ensure their financial and medical decisions are handled by a trusted person. For more information and to access the necessary forms, visit Texas Documents, where you can find resources to help you take this important step.
How to Become an Electrician in Iowa - Applicants must clearly print or type all required information in black or blue ink, ensuring legibility and accuracy.